
Piriformis syndrome (PS) is a rare neuromuscular condition that is related to inflammation of the sciatic nerve as it passes through or around the piriformis muscle, which is located deep in the buttock. There is frequently a delay in treatment of this condition, due to the fact that it can mimic facet arthritis, sacroilitis, hip osteoarthritis, trochanteric bursitis, sciatica and lumbar radiculopathy. Due to this delay, long-term nerve damage with persistent leg pain (including “tingling” “numbness” or “burning”), compensatory injuries and chronic weakness can occur.
Most people who develop Piriformis syndrome fall between 40 and 50 years of age, with women more commonly affected than men. It can occur following a direct blow to the buttock region or abnormal direct pressure in the region over time. This pressure can result from a wallet pressing against the buttock or asymmetrical sitting (sitting on one foot or sitting with the knees turned out). Other triggers include certain repetitive activities that require pivoting and extensive walking or running. Standing postures that adopt excessive “arch” in the lower back or hyperlordosis can cause an anterior tilt of the pelvis, internally rotate the hips and place excessive stretch on the Piriformis.
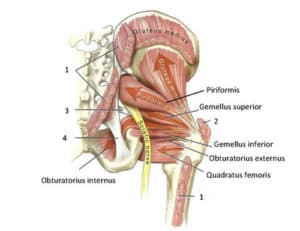
Anatomy of Piriformis Region
The origins of Piriformis syndrome are related to how the sciatic nerve runs under or through the muscle belly of the piriformis. In over 90% of the population, the nerve runs underneath the inferior portion of the piriformis. In over 20% of the patients, it runs through the piriformis muscle belly or splits. This anatomical variation results in a greater risk of developing Piriformis syndrome.
The piriformis muscle functions primarily as an external rotator of the hip that helps stabilize the sacrum and sacroiliac joint during walking and running. The piriformis muscle originates on the anterior medial surface of the sacrum inserting onto the greater trochanter. The primary nerve supply to the piriformis muscle comes from the nerve to piriformis sacral plexus S1 and S2.
Our Approach to Evaluation and Treatment
During evaluation, our first step is to take a thorough history of the patient’s condition that includes activities (both recreational and professional) that may contribute to the condition. We often want to know if there’s a particular incident or trauma that led up to the recent symptoms at the point of onset. Is there previous history of injuries to the lumbar spine sacroiliac joint or hip? Did the patient have any imaging (i.e. MRI, X-ray, CT Scan) and/or blood work? Oftentimes patients will arrive at the clinic prior to any screening for systemic problems or imaging. It is also not uncommon for patients to have already seen a practitioner or referring doctor who already started them on a course of anti-inflammatories, muscle relaxers, medications or a steroid-based medication or injection.
After a thorough history check, we often perform a clearing evaluation of the lumbar spine to ensure problem is not related to the lower lumbar spine. I often evaluate the lumbar spine first unless something in the history clearly points to a Piriformis hip or sacroiliac problem. Piriformis syndrome is the root of the problem in about 6-8% of cases of pain that is experienced in the back of the thigh occasionally extending below the knee, so it is important to look at the most common culprit first, the lumbar spine. At this point, if the lumbar spine, hip and sacroiliac joint has been evaluated and we don’t think it is contributing to the current patient complaints we take a closer look at the Piriformis being the source of pain.
Similar to many lumbar problems, you may have pain while sitting or going from sit to stand. However, in cases of Piriformis syndrome pain can also occur in lying and walking for longer than 30 minutes. Even in cases of Piriformis syndrome where you frequently change position, the subjective complaints of “sharp”, “burning”, “tingling” and/or “numbness” tend not to completely resolve as compared to lumbar pathologies. In addition to traditional symptoms in the buttock and posterior thigh region, patients will complain of groin, abdominal and pelvic pain. Generally, movement tends to reduce the pain in the buttock region. Many patients note pain that is one-sided, extending from and to the back of the knee. In some cases numbness may be reported in the foot.
Evaluation of A Suspected Piriformis
At first, when observing a patient walking, it can appear painful and the patient may display observable weakness in the form of “foot drop”, especially in chronic cases. In some cases, on the “painful side”, there is a significantly shortened limb (greater than ½ inch). Upon checking range of motion in the lower extremity, the patient has limited hip internal rotation. During strength testing, the external rotators and hip abductors demonstrate weakness and are painful. While placing direct pressure on the piriformis muscle belly, we may see thickening and muscular spasm. We perform special tests that put tension on the sciatic nerve and, in cases of PS, can reproduce the patient symptoms.
(Show Image of Toeing Out)
See our Next blog on treatment Options for Piriformis Syndrome!
If you are located in New Jersey and looking for a Wyckoff physical therapist, be sure that they provide a well-rounded rehabilitation program that will maximize your ability to gain full control and strength with your shoulder injury.
Apex Orthopedic Rehabilitation is a physical therapy center that has been providing physical therapy care to the Wyckoff, Ridgewood, Bergen County and surrounding towns.

Tom Willemann